This is an online E log book to discuss our patient’s de-identified data shared after taking his/her/guardian’s signed informed consent.”
FINAL EXAM LONG CASE
————————————————————————————
A 50 year old female patient a resident of Nalgonda, home maker came to the OPD with chief complaints of pain and stiffness in several joints since 1 year.
History of present illness:
She was apparently asymptomatic 10 years ago, then she developed a dull aching type of pain and stiffness in her finger joints(MCP joints) of right hand with limitations of movements at the joints.
Then within 6 months of onset the disease progressed to involve other joints of the right hand and left hand as well(wrist joint and elbow joint)
Within 4 years of onset she started feeling pain in the joints of the feet and ankle joint.
Since 3 months the pain became unbearable limiting her activities
The pain was insidious in onset, slowly progressive dull aching type of pain, non radiating, associated with swelling, stiffness and limitations of movements in the involved joints.
Stiffness and pain was more in the first 1 hour of waking up and gradually improved on movement.
There are few exacerbations associated with fever.
- No deformities
- No loss of weight.
- No involvement of distal interphalangeal joint
- No butterfly rash
- No abnormal jerky movements (chorea)
PAST HISTORY:
She has no similar complaints 10 years ago.
No history of thyroid, Asthma, hypertension, diabetes
DRUG HISTORY
No known drug allergies
MENSTRUAL HISTORY:
- Menarch: 13 years
- Regular 29 day cycles
- Menopause: 47 years
Family history:
No similar complaints
Personal history :
- Diet: mixed
- Appetite: normal
- Bowel and bladder: regular
- Sleep: adequate
- No addictions
General examination:
patient is conscious coherent and cooperative
Moderately built and nourished
- No edema
- No icterus
- No cyanosis
- No lymphadenopathy
- No pallor
VITALS:
- Temperature: a febrile
- Blood pressure: 115/70
- Respiratory rate: 15 CYCLES/MIN
- Pulse rate: 76bpm
LOCAL EXAMINATION:
INSPECTION
Skin :
No pigmentation
No scars
No atrophic changes
Nails: normal
Soft tissues: swelling over the joints
Deformities : no deformities

PALPATION
Skin: warm
Sensations are preserved
Soft tissues: no edema
Joint capsule: mild swelling over the joint
Tenderness over the joint (squeeze test)
Movements:
Decreased range of movements at PIP, MCP, wrist, elbow, ankle joints
All active and passive movements at the involved joints and painful.

EXTRA ARTICULAR MANIFESTATIONS:
Eye: no ocular manifestations (episcleritis, scleritis, keratoconjuctivitis sicca)
Ear: no hearing loss
Muscle: no muscle atrophy
GIT: no xerostomia, no parotid gland enlargement, no dysphasia
No lymphadenopathy
SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM
Apex beat: 5th intercostal space lateral to midclavicular line
S1 and s2 heard
JVP normal
Pedal edema: absent
RESPIRATORY SYSTEM
Breath sounds: normal
No additional breath sounds
CENTRAL NERVOUS SYSTEM
cranial nerves intact
Reflexes preserved
Sensations preserved
Joint position sense: intact
ABDOMEN
No abnormal findings found
DIFFERENTIAL DIAGNOSIS
1. Osteoarthritis
2. Rheumatoid arthritis
INVESTIGATIONS:
1. Complete blood picture
2. ESR
3. CRP
4. Rheumatoid factor
5. Liver function tests
6. Renal function tests
7. Urine examination
8. Antibodies
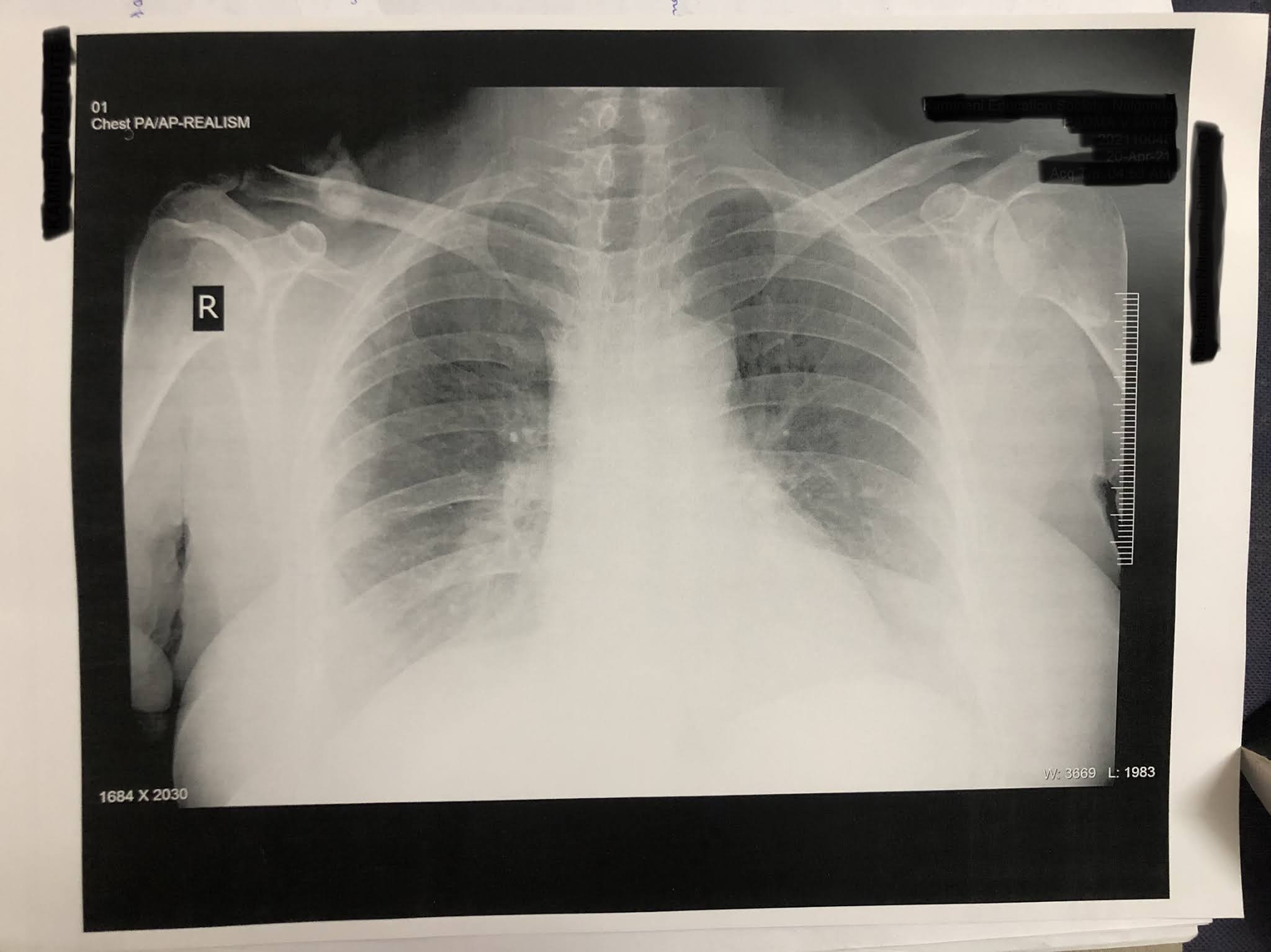
9. X-ray











No comments:
Post a Comment